Clinical Neuroanatomy Guide
Neuroanatomy
PNS & Spinal
Hindbrain
Fore & Midbrain
Clinical Terminology
- paralysis or plegia = loss of voluntary muscle control
- paresis = partial paralysis = weakness of voluntary muscle activity
- hypermetria = exaggerated protraction/retraction of the limb during gait
- ataxia = malposition of foot placements during gait
- intention tremor = involuntary oscillation of a body part(s) during posture or movement
- nystagmus = repetitive eye oscillation, typically eyes move more slowly away from center gaze then more quickly back to center. (NOTE: vestibular nystagmus is driven by imbalanced vestibular reflex activity, occurring normally during head acceleration & abnormally due to a lesion(s) having unilateral impact.)
- opisthotonus = severe persistent dorsally arched head and back; this can be the result of cerebellar cortical damage or strychnine poisoning. (opisthotonus = Gr. "drawn backward")
- neuromodulation - refers to the relatively prolonged excitatory or inhibitory influence of acetycholine, norepinephrine, dopamine, or serotonin on neuronal circuits. Most neuromodulation nuclei are found in the midbrain and pons. The nuclei are small, but axons from the nuclei are highly branched and widely distributed to broad regions of brain and spinal cord.
- paresis = partial paralysis = weakness of voluntary muscle activity
- hypermetria = exaggerated protraction/retraction of the limb during gait
- ataxia = malposition of foot placements during gait
- intention tremor = involuntary oscillation of a body part(s) during posture or movement
- nystagmus = repetitive eye oscillation, typically eyes move more slowly away from center gaze then more quickly back to center. (NOTE: vestibular nystagmus is driven by imbalanced vestibular reflex activity, occurring normally during head acceleration & abnormally due to a lesion(s) having unilateral impact.)
- opisthotonus = severe persistent dorsally arched head and back; this can be the result of cerebellar cortical damage or strychnine poisoning. (opisthotonus = Gr. "drawn backward")
- neuromodulation - refers to the relatively prolonged excitatory or inhibitory influence of acetycholine, norepinephrine, dopamine, or serotonin on neuronal circuits. Most neuromodulation nuclei are found in the midbrain and pons. The nuclei are small, but axons from the nuclei are highly branched and widely distributed to broad regions of brain and spinal cord.
Lower motor neurons
a single lower motor neuron is simultaneously known as a:
1. somatic efferent neuron located in a cranial nerve motor nucleus or in a motor nucleus within
the spinal cord ventral horn
2. motor unit neuron that innervates a collection of muscle fibers/cells within a skeletal muscle
3. final common pathway neuron responsible for muscle contraction, whether driven by
reflex activity and/or by voluntary action
• spinal lower motor neurons give rise to axons that run in spinal ventral roots & spinal nerves
• cranial nerve lower motor neurons send axons into cranial nerve roots attached to the brainstem:
midbrain -- oculomotor & trochlear nerves
pons -- trigeminal nerve
medulla oblongata – abducent (VI) through hypoglossal (XII) nerves
1. somatic efferent neuron located in a cranial nerve motor nucleus or in a motor nucleus within
the spinal cord ventral horn
2. motor unit neuron that innervates a collection of muscle fibers/cells within a skeletal muscle
3. final common pathway neuron responsible for muscle contraction, whether driven by
reflex activity and/or by voluntary action
• spinal lower motor neurons give rise to axons that run in spinal ventral roots & spinal nerves
• cranial nerve lower motor neurons send axons into cranial nerve roots attached to the brainstem:
midbrain -- oculomotor & trochlear nerves
pons -- trigeminal nerve
medulla oblongata – abducent (VI) through hypoglossal (XII) nerves
Upper motor neurons
Upper motor neurons are projection neurons that have their cell bodies within the brain. They give rise to descending tracts that terminate in cranial nerve motor nuclei or in spinal cord gray matter. The descending tracts are:
- for standing posture: pontine reticulospinal & lateral vestibulospinal (both run in the
spinal ventral funiculus)
- for voluntary movements: corticospinal, rubrospinal, and medullary reticuospinal tracts are used
(the first two decussate in the brain; all three run in the lateral funiculus).
NOTE: Typical voluntary movements simultaneously employ the following three tracts:
• medullary reticulospinal tract, which controls axial & proximal appendicular muscles
• rubrospinal tract, which controls proximal & mid-level appendicular joints
• lateral/ventral corticospinal tracts, which control carpus/tarsus & digits (corticospinal tracts are
more important for raccoons, least important for ungulates)
Upper neuron destruction syndrome: paralysis/paresis and, perhaps, extensor hypertonus
pending preservation of the standing posture tracts.
- for standing posture: pontine reticulospinal & lateral vestibulospinal (both run in the
spinal ventral funiculus)
- for voluntary movements: corticospinal, rubrospinal, and medullary reticuospinal tracts are used
(the first two decussate in the brain; all three run in the lateral funiculus).
NOTE: Typical voluntary movements simultaneously employ the following three tracts:
• medullary reticulospinal tract, which controls axial & proximal appendicular muscles
• rubrospinal tract, which controls proximal & mid-level appendicular joints
• lateral/ventral corticospinal tracts, which control carpus/tarsus & digits (corticospinal tracts are
more important for raccoons, least important for ungulates)
Upper neuron destruction syndrome: paralysis/paresis and, perhaps, extensor hypertonus
pending preservation of the standing posture tracts.
Spinal anatomy
Spinal white matter is divided bilaterally into three regions:
dorsal funiculus
- proprioception & discriminative touch pathways [damage results in ataxia & paw malposition]
lateral funiculus
- dorsal half: contains descending tracts for voluntary movement (rubrospinal, lateral corticospinal,
medullary reticulospinal)
- ventral half: contains the lateral spinothalamic pain pathway (pain also ascends bilaterally via
multiple tracts)
ventral funiculus
- conveys tracts for standing posture (pontine reticulospinal & lateral vestibulospinal tracts)
Spinal gray matter is divided bilaterally into three regions:
dorsal horn
- interneurons & ascending tract projection neurons that receive primary afferent input
intermediate substance (lateral horn, within segments T1 to L4)
- sympathetic preganglionic visceral efferent neuron cell bodies
ventral horn
- somatic efferent neuron cell bodies located in medial & lateral motor nuclei
(medial nuclei, which are present in all cord segments, innervate proximal muscles;
lateral nuclei, which are found in limb segments, innervate limb distal muscles)
dorsal funiculus
- proprioception & discriminative touch pathways [damage results in ataxia & paw malposition]
lateral funiculus
- dorsal half: contains descending tracts for voluntary movement (rubrospinal, lateral corticospinal,
medullary reticulospinal)
- ventral half: contains the lateral spinothalamic pain pathway (pain also ascends bilaterally via
multiple tracts)
ventral funiculus
- conveys tracts for standing posture (pontine reticulospinal & lateral vestibulospinal tracts)
Spinal gray matter is divided bilaterally into three regions:
dorsal horn
- interneurons & ascending tract projection neurons that receive primary afferent input
intermediate substance (lateral horn, within segments T1 to L4)
- sympathetic preganglionic visceral efferent neuron cell bodies
ventral horn
- somatic efferent neuron cell bodies located in medial & lateral motor nuclei
(medial nuclei, which are present in all cord segments, innervate proximal muscles;
lateral nuclei, which are found in limb segments, innervate limb distal muscles)
Hindbrain
Brainstem: pons & medulla oblongata:
- standing posture via the pontine reticulospinal tract & lateral vestibulospinal tract
Both tracts descend in the spinal ventral funiculus; also, descending tracts for
voluntary movement run through the hindbrain
- vestibular reflexes: maintain balanced posture of eyes, head, & limbs
- cranial nerve roots: trigeminal through hypoglossal nerve roots attach to the hindbrain
- visceral reflex centers (cardiovascular, respiratory, gastrointestinal, urinary, etc)
Cerebellum:
- vestibular role: the flocculonodular lobe interacts intimately with brainstem vestibular nuclei
- muscle tone: fastigial nucleus damage produces hypotonus (weakness); cerebellar cortex damage
leading to an uninhibitied fastigial nucleus produces opisthotonus.
- movement synergy: cerebellar hemisphere damage produces disturbance of movement amplitude &
strength: hypermetria, ataxia, trunk swaying, intention tremor (especially of the head)
- distance-rate-of-change perception: damage impairs visual menace response & avoidance
of running into walls, etc.
- standing posture via the pontine reticulospinal tract & lateral vestibulospinal tract
Both tracts descend in the spinal ventral funiculus; also, descending tracts for
voluntary movement run through the hindbrain
- vestibular reflexes: maintain balanced posture of eyes, head, & limbs
- cranial nerve roots: trigeminal through hypoglossal nerve roots attach to the hindbrain
- visceral reflex centers (cardiovascular, respiratory, gastrointestinal, urinary, etc)
Cerebellum:
- vestibular role: the flocculonodular lobe interacts intimately with brainstem vestibular nuclei
- muscle tone: fastigial nucleus damage produces hypotonus (weakness); cerebellar cortex damage
leading to an uninhibitied fastigial nucleus produces opisthotonus.
- movement synergy: cerebellar hemisphere damage produces disturbance of movement amplitude &
strength: hypermetria, ataxia, trunk swaying, intention tremor (especially of the head)
- distance-rate-of-change perception: damage impairs visual menace response & avoidance
of running into walls, etc.
Midbrain
The midbrain contains:
- reticular activating system provides background excitation to the cerebral cortex to preclude coma;
also, neuromodulation nuclei in the midbrain (& pons) influence mood, movement, pain sensitivity.
- red nucleus, gives rise to axons that immediately decussate and descend as the rubrospinal tract
NOTE: In quadrupeds, the rubrospinal is the major tract for voluntary movement (including
suppression of default standing posture during limb flexion). Pending lesion location,
a unilateral lesion may cause ipsilateral (rubrospinal tract) or contralateral (red nucleus)
paresis/paralysis.
- corticospinal fibers run through the midbrain, prior to decussating in the medulla oblongata
- cranial nerve nuclei and roots:
oculomotor nerve (enables eye movement medially & pupil constriction)
trochlear nerve (innervates dorsal oblique m.)
- tectum: orientation of head, eyes & ears toward a sudden auditory or visual stimulus:
vision involves the rostral colliculus & hearing involves the caudal colliculus
- pretectal region: pupillary light reflex
- periaqueductal gray: relays visceral information and gives rise to an endogenous analgesia system
that suppresses pain pathway traffic.
- reticular activating system provides background excitation to the cerebral cortex to preclude coma;
also, neuromodulation nuclei in the midbrain (& pons) influence mood, movement, pain sensitivity.
- red nucleus, gives rise to axons that immediately decussate and descend as the rubrospinal tract
NOTE: In quadrupeds, the rubrospinal is the major tract for voluntary movement (including
suppression of default standing posture during limb flexion). Pending lesion location,
a unilateral lesion may cause ipsilateral (rubrospinal tract) or contralateral (red nucleus)
paresis/paralysis.
- corticospinal fibers run through the midbrain, prior to decussating in the medulla oblongata
- cranial nerve nuclei and roots:
oculomotor nerve (enables eye movement medially & pupil constriction)
trochlear nerve (innervates dorsal oblique m.)
- tectum: orientation of head, eyes & ears toward a sudden auditory or visual stimulus:
vision involves the rostral colliculus & hearing involves the caudal colliculus
- pretectal region: pupillary light reflex
- periaqueductal gray: relays visceral information and gives rise to an endogenous analgesia system
that suppresses pain pathway traffic.
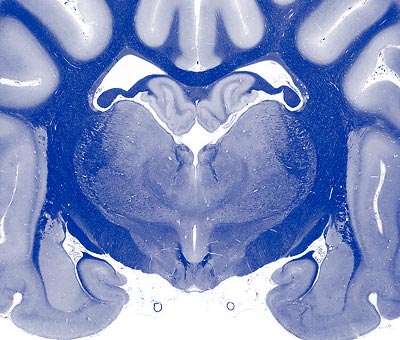
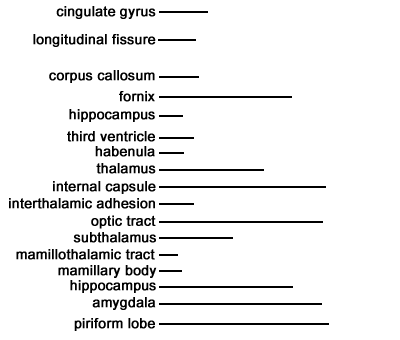
Diencephalon
The diencephalon includes the thalamus, hypothalamus, subthalamus, and epithalamus.
- subthalamus: used by the cerebral cortex to suppress unwanted movements (the subthalamus
excites inhibitory neurons located within basal nuclei).
- epithalamus: involved in threat induced inhibition of movement (movement freeze behavior).
- thalamic nuclei: all ascending tracts destined for the neocortex relay in a thalamic nucleus,
including pathways from the cerebellum and axons arising from basal nuclei.
- vision: lateral geniculate nucleus relays conscious vision to the neocortex pretectal region
processes reflex pupil constriction (via oculomotor nerve) optic tract destruction produces
contralateral blindness in the visual fields of both eyes optic nerve destruction produces
complete blindness of the ipsilateral eye
- hearing: medial geniculate nucleus relays conscious hearing to the neocortex.
- hypothalamus: autonomic control, including visceral responses related to emotional states,
pituitary gland control, and visceral related responses/behavior, including: eating, drinking,
temperature regulation and circadian rhythms linked to daylight.
- subthalamus: used by the cerebral cortex to suppress unwanted movements (the subthalamus
excites inhibitory neurons located within basal nuclei).
- epithalamus: involved in threat induced inhibition of movement (movement freeze behavior).
- thalamic nuclei: all ascending tracts destined for the neocortex relay in a thalamic nucleus,
including pathways from the cerebellum and axons arising from basal nuclei.
- vision: lateral geniculate nucleus relays conscious vision to the neocortex pretectal region
processes reflex pupil constriction (via oculomotor nerve) optic tract destruction produces
contralateral blindness in the visual fields of both eyes optic nerve destruction produces
complete blindness of the ipsilateral eye
- hearing: medial geniculate nucleus relays conscious hearing to the neocortex.
- hypothalamus: autonomic control, including visceral responses related to emotional states,
pituitary gland control, and visceral related responses/behavior, including: eating, drinking,
temperature regulation and circadian rhythms linked to daylight.
Cerebrum
The cerebrum is composed of bilateral cerebral hemishperes. Cerebral gray matter is either superficial (cerebral cortex) or buried (basal nuclei). The term rhinencephalon refers to the older, ventral cerebrum that is concerned with olfaction, emotions, and recent memory. The dorsal cerebrum is covered by six-layered neocortex:
- neocortex is essential for consciousness & mental alertness, intelligence & learning, pattern recognition & cognition, self-awareness & comprehension of significance, memory storage & recall, planning & appropriate behavior, and selecting & executing voluntary movement.
- neocortical regions:
primary sensory areas (somatosensory, visual, auditory, etc.) - receive thalamic sensory projections
sensory association cortex (surrounds primary areas) - extracts pattern/significance from sensations
prefrontal association cortex (frontal pole) - plans/directs goal-oriented focused behavior
premotor cortex - involved in movement selection and motor learning
motor cortex - somatotopic organization of joint movements; drives pyramidal/extrapyramidal tracts
- basal nuclei [caudate, putamen, & globus pallidus] participate in inhibitory circuits
that suppress undesired components of voluntary movement.
- limbic system structures (e.g., cingulate gyrus, septum, nucleus accumbens, amygdala, hippocampus) process emotional reactions that drive memory and behavior (e.g., self-defense, escape, mating, etc.); limbic system also includes components of the diencephalon and midbrain.
- olfactory neurons synapse in the olfactory bulb, which sends axons to the piriform lobe for conscious olfaction and to the limbic system for emotional responses (e.g., pheromones elicit emotionally driven behavior).
- neocortex is essential for consciousness & mental alertness, intelligence & learning, pattern recognition & cognition, self-awareness & comprehension of significance, memory storage & recall, planning & appropriate behavior, and selecting & executing voluntary movement.
- neocortical regions:
primary sensory areas (somatosensory, visual, auditory, etc.) - receive thalamic sensory projections
sensory association cortex (surrounds primary areas) - extracts pattern/significance from sensations
prefrontal association cortex (frontal pole) - plans/directs goal-oriented focused behavior
premotor cortex - involved in movement selection and motor learning
motor cortex - somatotopic organization of joint movements; drives pyramidal/extrapyramidal tracts
- basal nuclei [caudate, putamen, & globus pallidus] participate in inhibitory circuits
that suppress undesired components of voluntary movement.
- limbic system structures (e.g., cingulate gyrus, septum, nucleus accumbens, amygdala, hippocampus) process emotional reactions that drive memory and behavior (e.g., self-defense, escape, mating, etc.); limbic system also includes components of the diencephalon and midbrain.
- olfactory neurons synapse in the olfactory bulb, which sends axons to the piriform lobe for conscious olfaction and to the limbic system for emotional responses (e.g., pheromones elicit emotionally driven behavior).
Peripheral nerve syndrome
- damage may be severe but it is limited to structures innervated by particular affected nerve(s)
- resultant paralysis is flaccid, includings areflexia involving muscles innervated by affected nerve(s)
- severe and relatively rapid (days) atrophy of muscles innervated by affected nerve(s)
- anesthesia of skin fields innervated by cutaneous branches of the affected nerve(s)
- resultant paralysis is flaccid, includings areflexia involving muscles innervated by affected nerve(s)
- severe and relatively rapid (days) atrophy of muscles innervated by affected nerve(s)
- anesthesia of skin fields innervated by cutaneous branches of the affected nerve(s)
Cauda equina spinal syndrome (sacral & caudal segments)
- flaccid paralysis, muscle atrophy, and skin anesthesia involving the tail
- cutaneous anesthesia of the perineum including the anal region
- fecal and urinary incontinence
- enlarged atonic bladder with urine overflow
- cutaneous anesthesia of the perineum including the anal region
- fecal and urinary incontinence
- enlarged atonic bladder with urine overflow
Lumbosacral spinal syndrome (L4 – S1)
due to local spinal cord damage:
- pelvic limb muscles exhibit flaccid paralysis, areflexia, and muscle atrophy
- pelvic limb exhibits areas of skin anesthesia
due to spinal tract damage:
- tail exhibits voluntary paralysis and anesthesia of conscious sensation
- voluntary urinary incontinence; incomplete urination with residual urine retention
(detrusor-sphincter dyssynergy)
- pelvic limb muscles exhibit flaccid paralysis, areflexia, and muscle atrophy
- pelvic limb exhibits areas of skin anesthesia
due to spinal tract damage:
- tail exhibits voluntary paralysis and anesthesia of conscious sensation
- voluntary urinary incontinence; incomplete urination with residual urine retention
(detrusor-sphincter dyssynergy)
Thoracolumbar spinal syndrome (T3 – L3)
due to spinal tract damage:
- absence of cutaneous trunci reflex and cutaneous conscious sensation caudal to the lesion
- pelvic limb & tail: voluntary paralysis and anesthesia of conscious sensation
- pelvic limb: absence of postural reactions (e.g., proprioception, hopping, etc.);
spinal reflexes present, including appearance of the abnormal withdrawal-crossed extension;
extensor muscle hypertonus may exist (pending the nature of tract damage)
- extensor hypertonus may be evident in thoracic limbs due to loss of inhibition from pelvic limbs
- voluntary urinary incontinence; incomplete urination with residual urine retention
(detrusor-sphincter dyssynergy)
- absence of cutaneous trunci reflex and cutaneous conscious sensation caudal to the lesion
- pelvic limb & tail: voluntary paralysis and anesthesia of conscious sensation
- pelvic limb: absence of postural reactions (e.g., proprioception, hopping, etc.);
spinal reflexes present, including appearance of the abnormal withdrawal-crossed extension;
extensor muscle hypertonus may exist (pending the nature of tract damage)
- extensor hypertonus may be evident in thoracic limbs due to loss of inhibition from pelvic limbs
- voluntary urinary incontinence; incomplete urination with residual urine retention
(detrusor-sphincter dyssynergy)
Cervicothoracic spinal syndrome (C6 – T2)
due to local spinal cord damage:
- thoracic limb muscles exhibit flaccid paralysis, areflexia, and muscle atrophy
- thoracic limb exhibits areas of skin anesthesia
due to spinal tract damage:
- trunk, pelvic limb & tail: exhibit voluntary paralysis and anesthesia of conscious sensation
- pelvic limb: absence of postural reactions (e.g., proprioception, hopping, etc.);
spinal reflexes present, including appearance of the abnormal withdrawal-crossed extension;
extensor muscle hypertonus may exist (pending the nature of tract damage)
- voluntary incontinence; incomplete urination with residual urine retention
(detrusor-sphincter dyssynergy)
- thoracic limb muscles exhibit flaccid paralysis, areflexia, and muscle atrophy
- thoracic limb exhibits areas of skin anesthesia
due to spinal tract damage:
- trunk, pelvic limb & tail: exhibit voluntary paralysis and anesthesia of conscious sensation
- pelvic limb: absence of postural reactions (e.g., proprioception, hopping, etc.);
spinal reflexes present, including appearance of the abnormal withdrawal-crossed extension;
extensor muscle hypertonus may exist (pending the nature of tract damage)
- voluntary incontinence; incomplete urination with residual urine retention
(detrusor-sphincter dyssynergy)
Cervical spinal syndrome (C1 – C5)
due to local spinal cord damage:
- anesthesia of cervical skin & possible evidence of neck muscle atrophy
due to spinal tract damage:
- voluntary paralysis and anesthesia of conscious sensation caudal to the lesion
- thoracic & pelvic limbs: absence of postural reactions (e.g., proprioception, hopping, etc.);
spinal reflexes present, including appearance of the abnormal withdrawal-crossed extension;
extensor muscle hypertonus may exist (pending the nature of tract damage)
- voluntary urinary incontinence; incomplete urination with residual urine retention
(detrusor-sphincter dyssynergy)
- anesthesia of cervical skin & possible evidence of neck muscle atrophy
due to spinal tract damage:
- voluntary paralysis and anesthesia of conscious sensation caudal to the lesion
- thoracic & pelvic limbs: absence of postural reactions (e.g., proprioception, hopping, etc.);
spinal reflexes present, including appearance of the abnormal withdrawal-crossed extension;
extensor muscle hypertonus may exist (pending the nature of tract damage)
- voluntary urinary incontinence; incomplete urination with residual urine retention
(detrusor-sphincter dyssynergy)
Brainstem
- damage to cranial nerves can indicate the level(s) of brainstem lesion(s):
trigeminal nerve [pons]: loss of face sensation & paralysis of muscle of mastication
abducent nerve [rostral medulla]: medial strabismus (nerve runs forward to the orbital fissure)
facial nerve [rostral medulla]: paralysis of facial expression, drooped lips
vestibulocochlear nerve [rostral medulla]: vestibular syndrome; unilateral deafness
glossopharyngeal nerve [caudal medulla]: impaired gag reflexes and pharyngeal sensation
vagus nerve [caudal medulla]: paralysis of pharynx and larynx (gag reflexes)
hypoglossal nerve [caudal medulla]: tongue paralysis, atrophy & deviation toward lesion side
- damage to cranial nerve nuclei could produce more diffuse cranial nerve signs
- damage to autonomic centers could impact respiration, heart rate, etc.
- damage to descending tracts that originate and/or pass through the hindbrain:
pontine reticululospinal & lateral vestibulospinal: ipsilateral falling (extensor hypo-tonus)
rubrospinal tract: ipsilateral joint flexion paralysis of thoracic & pelvic limbs
pyramidal tract: contralateral weakness of manus & pes, especially navigating steps
trigeminal nerve [pons]: loss of face sensation & paralysis of muscle of mastication
abducent nerve [rostral medulla]: medial strabismus (nerve runs forward to the orbital fissure)
facial nerve [rostral medulla]: paralysis of facial expression, drooped lips
vestibulocochlear nerve [rostral medulla]: vestibular syndrome; unilateral deafness
glossopharyngeal nerve [caudal medulla]: impaired gag reflexes and pharyngeal sensation
vagus nerve [caudal medulla]: paralysis of pharynx and larynx (gag reflexes)
hypoglossal nerve [caudal medulla]: tongue paralysis, atrophy & deviation toward lesion side
- damage to cranial nerve nuclei could produce more diffuse cranial nerve signs
- damage to autonomic centers could impact respiration, heart rate, etc.
- damage to descending tracts that originate and/or pass through the hindbrain:
pontine reticululospinal & lateral vestibulospinal: ipsilateral falling (extensor hypo-tonus)
rubrospinal tract: ipsilateral joint flexion paralysis of thoracic & pelvic limbs
pyramidal tract: contralateral weakness of manus & pes, especially navigating steps
Vestibular syndromes
Vestibular syndromes result from damage affecting the labyrinth, vestibular nerve, brainstem, and/or cerebellum. Vestibular syndromes represent the brain’s reflex response to a persistent right/left vestibular imbalance, caused by a lesion instead of head acceleration.
Typically, the direction of clinical signs reveals which side is damaged and the severity of the clinical signs reflects the severity of destruction. Clinical signs comprising the vestibular syndrome include:
- head tilt [down ear toward the damaged side]
- stumbling, falling, rolling [toward the damaged side]
- nystagmus [slow phase toward the damaged side] (nystagmus in a vertical direction,
as opposed to horizontal, is indicative of lesion located within the brain)
Untypically, clinical signs are directed toward the normal (non-lesion) side. Called paradoxical vestibular syndrome this could result from cerebellar damage, loss of inhibition allowing more excitation on the lesion side.
Typically, the direction of clinical signs reveals which side is damaged and the severity of the clinical signs reflects the severity of destruction. Clinical signs comprising the vestibular syndrome include:
- head tilt [down ear toward the damaged side]
- stumbling, falling, rolling [toward the damaged side]
- nystagmus [slow phase toward the damaged side] (nystagmus in a vertical direction,
as opposed to horizontal, is indicative of lesion located within the brain)
Untypically, clinical signs are directed toward the normal (non-lesion) side. Called paradoxical vestibular syndrome this could result from cerebellar damage, loss of inhibition allowing more excitation on the lesion side.
Cerebellar syndromes
The cerebellar cortex inhibits cerebellar nuclei. Axons from the nuclei exit the cerebellum and massively excite motor nuclei. Thus, cerebellar cortex damage results in exaggerated muscle tone / movement and cerebellar nuclei damage results in hypotonia / weakness syndromes.
Clinical signs typical of a cerebellar syndrome include:
- wide based stance (required to maintain balance during standing)
- ataxic gait (limb foot fall placement is inconsistent and malpositioned)
- hypermetric gait (limbs are protracted too high and slammed down too hard)
- intention tremor (e.g., head tremor is seen when the head is not resting on the ground)
- menace response deficiency (distance judgment of an approaching object is impaired)
Clinical signs typical of a cerebellar syndrome include:
- wide based stance (required to maintain balance during standing)
- ataxic gait (limb foot fall placement is inconsistent and malpositioned)
- hypermetric gait (limbs are protracted too high and slammed down too hard)
- intention tremor (e.g., head tremor is seen when the head is not resting on the ground)
- menace response deficiency (distance judgment of an approaching object is impaired)
Midbrain syndromes
Destructive lesions of the midbrain would be expected to produce:
- paresis/paralysis of the limbs due to red nucleus damage -- contralateral paralysis occurs when the
damage is rostral to the rubrospinal tract decussation in the caudal midbrain;
damage to corticospinal axons in the crus cerebri would affect the contralateral manus/pes.
- lateral strabismus and ipsilateral loss of the pupillary light reflex would result from
oculomotor nerve/nucleus damage
- orientation of the head, eyes & ears toward a sudden visual (rostral colliculus) or
auditory (caudal colliculus) stimulus could be affected by tectum damage
- coma may result from destruction of the reticular activating system (which generates background
excitation for the cerebral cortex)
- paresis/paralysis of the limbs due to red nucleus damage -- contralateral paralysis occurs when the
damage is rostral to the rubrospinal tract decussation in the caudal midbrain;
damage to corticospinal axons in the crus cerebri would affect the contralateral manus/pes.
- lateral strabismus and ipsilateral loss of the pupillary light reflex would result from
oculomotor nerve/nucleus damage
- orientation of the head, eyes & ears toward a sudden visual (rostral colliculus) or
auditory (caudal colliculus) stimulus could be affected by tectum damage
- coma may result from destruction of the reticular activating system (which generates background
excitation for the cerebral cortex)
Diencephalon syndromes
Destructive lesions of the diencephalon would be expected to produce:
- crying behavior (apparently due to pain) has been observed with thalamic infarct lesions
- conscious sensation deficits (sensory information is relayed to the neocortex through the thalamus)
- blindness:
optic nerve damage: the ipsilateral eye is blind & its pupillary light reflex is absent
optic tract or lateral geniculate nucleus damage: contralateral sides of visual fields are blind for
both eyes; pupillary light reflexes are not impaired
- endocrine disorders, due to hypothalamus & pituitary damage
- autonomic disorders due to hypothalamus damage,
related to eating, drinking, temperature regulation, circadian rhythms, etc.
- crying behavior (apparently due to pain) has been observed with thalamic infarct lesions
- conscious sensation deficits (sensory information is relayed to the neocortex through the thalamus)
- blindness:
optic nerve damage: the ipsilateral eye is blind & its pupillary light reflex is absent
optic tract or lateral geniculate nucleus damage: contralateral sides of visual fields are blind for
both eyes; pupillary light reflexes are not impaired
- endocrine disorders, due to hypothalamus & pituitary damage
- autonomic disorders due to hypothalamus damage,
related to eating, drinking, temperature regulation, circadian rhythms, etc.
Cerebral syndromes
Destructive lesions of the cerebrum could produce:
- mental impairment -- depressed alertness & decreased interaction with surroundings;
impaired intelligence & deficient learning/learned behavior, including housetrained behavior
- voluntary movement deficiency -- head pressing, pacing (wide-circling toward lesion side)
spastic paralysis (damage to cerebral cortex-basal nuclei-thalamus-motor cortex circuit)
- conscious sensation impairment (blindness, loss of voice recognition, etc.)
- goal-directed behavior deterioration, resulting from damage to the frontal lobe (prefrontal cortex)
(short term memory deficits, inability to ignore distractions, control emotions to achieve a goal)
- neglect syndrome (parts of a patient's own body are regarded as foreign by the patient)
- seizures
- mood alteration (for example, uncharacteristic aggression or docility)
Note: Lesions in one cerebral hemisphere produce contralateral motor/sensory deficits.
- mental impairment -- depressed alertness & decreased interaction with surroundings;
impaired intelligence & deficient learning/learned behavior, including housetrained behavior
- voluntary movement deficiency -- head pressing, pacing (wide-circling toward lesion side)
spastic paralysis (damage to cerebral cortex-basal nuclei-thalamus-motor cortex circuit)
- conscious sensation impairment (blindness, loss of voice recognition, etc.)
- goal-directed behavior deterioration, resulting from damage to the frontal lobe (prefrontal cortex)
(short term memory deficits, inability to ignore distractions, control emotions to achieve a goal)
- neglect syndrome (parts of a patient's own body are regarded as foreign by the patient)
- seizures
- mood alteration (for example, uncharacteristic aggression or docility)
Note: Lesions in one cerebral hemisphere produce contralateral motor/sensory deficits.
Interpreting neurological exams (diagnosing probable locations of destructive lesions) requires pertinent knowledge of clinical neuroanatomy.
This web page concisely details clinical neuroanatomy and neurological syndromes pertinent to the neurological exam. It is intended for students and clinicians who wish to review their neurological knowledge.
Exit to Locating Neurological Lesions Exercises
Exit to Locate Neurological Lesions Guide
(smart phone web app)
Exit to Veterinary Anatomy Website
Click/Tap
